- Femur
- Knee Joint
- Muscles
- Femoral Triangle
- Innervation
- Arteries, Lymphatics & Veins
- Knee Complex
- Study Questions
The bone between the hip and the knee is the femur. It is the longest and strongest bone in the body. The femur articulates proximally with the acetabulum and distally with the tibia and patella.
The knee joint is formed by articulations of the femur, tibia, and patella. The knee joint enables flexion, extension, and minimal rotation of the femur and tibia.




Actions of the Knee Complex
The articulations between the femur, tibia, and patella form the knee joint and enable the following actions

A. Actions of the knee joint. B. Compartments of the thigh. C. Muscles of the anterior compartment of the thigh.
- Flexion. Movement in the sagittal plane, decreasing the knee joint angle.
- Extension. Movement in the sagittal plane, increasing the knee joint angle.
- Medial rotation. Movement toward the midline in the transverse or axial plane.
- Lateral rotation. Movement away from the midline in the transverse or axial plane.
The muscles of the thigh are divided by their fascial compartments (anterior, medial, and posterior) and may cross the hip or knee joint. Identifying which joints the muscles cross and the side on which they cross can provide useful insight into the actions of these muscles.
Muscle |
Proximal Attachment |
Distal Attachment |
Action |
Innervation |
|---|---|---|---|---|
Anterior compartment of the thigh |
||||
Psoas minor |
T12–L1 vertebral bodies and discs |
Pectin pubis |
Lumbar spine flexion, posterior pelvic tilt |
Anterior rami (L1) |
Psoas major |
T12–L5 transverse processes, vertebral bodies and discs |
Lesser trochanter of femur |
Flexes and externally rotates thigh at hip joint; flexes trunk (psoas major) |
Anterior rami (L1–L3) |
Iliacus |
Iliac fossa |
Femoral n. (L2, L3) |
||
Sartorius |
Anterior superior iliac spine |
Inferomedial to tibial tuberosity (pes anserinus) |
Flexes thigh at hip joint and flexes leg at knee joint |
Femoral n. (L2, L3) |
Rectus femoris |
Anterior inferior iliac spine |
Flexes thigh at hip joint and extends leg at knee joint |
Femoral n. (L2–L4) |
|
Vastus lateralis |
Lateral part of intertrochanteric line, margin of greater trochanter, lateral margin of gluteal tuberosity, lateral lip of linea aspera |
Quadriceps femoris tendon |
Extends leg at knee joint |
|
Vastus medialis |
Medial part of intertrochanteric line, pectineal line, medial lip of linea aspera, medial supracondylar ridge |
|||
Vastus intermedius |
Femur: upper two-thirds of anterior and lateral surfaces |
|||
Medial compartment of the thigh |
||||
Pectineus |
Pectineal line |
Oblique line extending from base of lesser trochanter to linea aspera on posterior surface of proximal femur |
Adducts and flexes thigh at hip joint |
Femoral n. (L2, L3) |
Adductor longus |
Body of pubis |
Linea aspera |
Adducts and medially rotates thigh at hip joint |
Obturator n. (anterior division) (L2–L4) |
Adductor brevis |
Body of pubis and inferior pubic ramus |
Obturator n. (anterior division) (L2, L3) |
||
Adductor magnus |
Adductor part: ischiopubic ramus Hamstring part: ischial tuberosity |
Adductor part: linea aspera Hamstring part: Adductor tubercle |
Adducts and medially rotates thigh at hip joint |
Adductor part: obturator n. (L2–L4) Hamstring part: tibial division of sciatic n. (L4) and obturator n. (L2, L3) |
Gracilis |
Body and inferior ramus of pubic bone |
Medial surface of proximal shaft of tibia (pes anserinus) |
Adducts thigh at hip joint and flexes leg at knee joint |
Obturator n. (L2, L3) |
Obturator externus |
External surface of obturator membrane and adjacent bone |
Trochanteric fossa |
Laterally rotates hip |
Obturator n. (posterior division) (L3, L4) |
Posterior compartment of the thigh |
||||
Semitendinosus |
Ischial tuberosity |
Medial surface of proximal tibia (pes anserinus) |
Flexes leg at knee joint and extends thigh at hip joint; medially rotates thigh at hip joint and leg at knee joint |
Tibial division of sciatic n. (L5–S2) |
Semimembranosus |
Medial and posterior surface of medial tibial condyle |
|||
Biceps femoris |
Long head: ischial tuberosity Short head: lateral lip of linea aspera |
Head of fibula |
Knee flexion Hip extension Lateral rotation of hip and knee |
Long head: tibial division of sciatic n. (L5–S2) Short head: common fibular division of sciatic n. (L5–S2) |
Muscles of the Anterior Compartment of the Thigh
The muscles in the anterior compartment of the thigh are primarily flexors of the hip or extensors of the knee because of their anterior orientation (Figure 36-1C). The femoral nerve (L2–L4) innervates these muscles; however, each muscle does not necessarily receive each spinal nerve level between L2 and L4.
- Iliopsoas musculature. Originates from two muscles, the psoas major and iliacus muscles, which join to form a common tendon. The psoas major muscle attaches along vertebrae T12–L5, discs, and the iliacus within the iliac fossa. Both the psoas and iliacus muscles join together as they course deep to the inguinal ligament and insert onto the lesser trochanter of the femur. The main action of these muscles is to flex and laterally rotate the thigh at the hip joint. Innervation to the psoas major muscle is via the anterior rami of L1, L2, and L3, whereas innervation to the iliacus is through the femoral nerve (anterior rami of L2 and L3).
- Sartorius muscle. Attaches proximally to the anterior superior iliac spine. The distal insertion of the sartorius muscle is medial to the tibial tuberosity, contributing to the pes anserinus. Pes anserinus (“goose's foot”) is a term used to describe the conjoined tendons of the sartorius, gracilis, and semitendinosus muscles; their common insertion is medial to the tibial tuberosity. The action of the sartorius muscle is to flex, abduct, and laterally rotate the thigh at the hip joint and flex the leg at the knee joint. The femoral nerve (L2 and L3) innervates this muscle.
- Quadriceps femoris muscle group. A four-headed muscle in the anterior compartment of the thigh and is a strong extensor muscle of the knee. There are four separate muscles in this group, each with distinct origins. However, all four parts of the quadriceps femoris muscle attach to the patella, via the quadriceps tendon, and then insert onto the tibial tuberosity. The femoral nerve (L2–L4) innervates the quadriceps femoris muscle group. The four separate muscles are as follows:
- Rectus femoris muscle. Attaches on the anterior inferior iliac spine and to the quadriceps femoris tendon. The rectus femoris muscle flexes the thigh at the hip joint and extends the leg at the knee joint.
- Vastus lateralis muscle. Attaches proximally at the intertrochanteric line and the lateral lip of the linea aspera; distally, the muscle attaches to the quadriceps femoris tendon. The vastus lateralis muscle extends the leg at the knee joint.
- Vastus medialis muscle. Attaches proximally at the intertrochanteric line and the lateral lip of the linea aspera; distally, the muscle attaches to the quadriceps femoris tendon. The vastus medialis muscle extends the leg at the knee joint.
- Vastus intermedius muscle. Attaches proximally along the anterior and lateral surfaces of the upper two-thirds of the femoral shaft; distally, the muscle attaches to the quadriceps femoris tendon. The vastus intermedius muscle extends the leg at the knee joint.
The muscles in the medial compartment of the thigh are primarily adductors of the hip because of their medial orientation. The obturator nerve (L2–L4) innervates most of the muscles in the medial compartment of the thigh. However, each muscle does not necessarily receive each spinal nerve level between L2 and L4 (Figure 36-2A and B).
- Pectineus muscle. Attaches to the pectineal line of the pubis and the posterior surface of the proximal femur. The pectineus muscle adducts and flexes the thigh at the hip joint. The femoral nerve (L2 and L3) innervates this muscle, with occasional branches from the obturator nerve.
- Adductor longus muscle. Attaches proximally to the body of the pubis; distally, the muscle attaches on the linea aspera. The adductor longus muscle adducts and medially rotates the thigh at the hip joint. The obturator nerve (L2–L4) innervates this muscle.
- Adductor magnus muscle. Consists of an adductor part and a hamstring part. Proximally, the adductor part attaches to the ischiopubic ramus, and the hamstring part attaches to the ischial tuberosity. Distally, the adductor part of the muscle attaches on the linea aspera, and the hamstring part attaches on the adductor tubercle. The adductor magnus muscle is the largest and deepest muscle of the muscles of the medial compartment of the thigh. It adducts and medially rotates the thigh at the hip joint. The obturator nerve (L2–L4) innervates the adductor part of the muscle, and the tibial division of the sciatic nerve (L4) and the obturator nerve (L2 and L3) innervate the hamstring part of the muscle.
- Adductor brevis muscle. Attaches proximally to the inferior pubic ramus and the linea aspera. The adductor brevis muscle adducts and medially rotates the thigh at the hip joint. The obturator nerve (L2–L4) innervates this muscle.
- Gracilis muscle. Attaches to the inferior pubic ramus and the medial surface of the proximal shaft of the tibia (pes anserinus). The gracilis muscle adducts the thigh at the hip joint and flexes the leg at the knee joint. The obturator nerve (L2 and L3) innervates this muscle.
- Obturator externus muscle. Attaches to the external surface of the obturator membrane, adjacent bone, and trochanteric fossa. The obturator externus muscle laterally rotates the femur at the hip joint. The obturator nerve (L3 and L4) innervates this muscle.

A. Superficial view of muscles of the medial compartment of the thigh. B. Deep view of muscles of the medial compartment of the thigh. C. Muscles of the posterior compartment of the thigh (hamstrings).
Muscles of the Posterior Compartment of the Thigh
The muscles in the posterior compartment of the thigh are primarily extensors of the hip or flexors of the knee because of their posterior orientation. The tibial nerve (L4–S3) innervates the muscles in the posterior compartment of the thigh, with the exception of the short head of the biceps femoris muscles (common fibular nerve). Muscles in this compartment do not receive all the innervation levels from the tibial nerve; rather, they receive innervation from the spinal nerve level between L5 and S2 (Figure 36-2C).
- Semitendinosus muscle. Attaches proximally to the ischial tuberosity and the medial surface of the proximal tibia (pes anserinus). The semitendinosus muscle extends and medially rotates the thigh at the hip joint. In addition, the muscle flexes and medially rotates the leg at the knee joint. The tibial division of the sciatic nerve (L5–S2) innervates this muscle.
- Semimembranosus muscle. Attaches proximally to the ischial tuberosity and the medial tibial condyle. The semimembranosus muscle flexes and medially rotates the leg at the knee joint and extends and medially rotates the thigh at the hip joint. The tibial division of the sciatic nerve (L5–S2) innervates this muscle.
- Biceps femoris muscle. Consists of two heads (long and short heads). Proximally, the long head attaches on the ischial tuberosity, and the short head attaches to the lateral lip of the linea aspera. Distally, the muscle attaches to the head of the fibula. The biceps femoris muscle flexes and medially rotates the leg at the knee joint and extends and medially rotates the thigh at the hip joint. The tibial nerve (L5–S2) innervates the long head, and the short head is innervated by the common fibular nerve (L5–S2).
The femoral triangle is an area in the inguinal region that is shaped like an upside-down triangle. The femoral triangle contains the femoral nerve, artery, and vein, and the lymphatics. The femoral triangle is an area in the inguinal region that is shaped like an upside-down triangle and is bordered by the sartorius muscle, adductor longus muscle and inguinal ligament. The femoral triangle contains the following structures from lateral to medial (Figure 36-3A):
- Femoral nerve. Originates as a branch of the lumbar plexus. The femoral nerve is not contained within the femoral sheath.
- Femoral artery. Continuation of the external iliac artery. The femoral artery is located midway between the anterior superior iliac spine and the pubic symphysis.
- Femoral vein. Continues as the external iliac vein.
- Lymphatics.

A. Femoral triangle. B. Innervation of the compartments of the thigh. C. Femoral nerve.
Often, the acronym NAVL is used to represent the orientation of the structures of the femoral triangle. The inferior portion of the femoral triangle communicates with a facial canal (adductor canal) that runs deep to the sartorius muscle.
The lower limb is innervated by the ventral rami from nerve roots L1–S4, which form two separate networks of nerves that are referred to as the lumbar plexus (L1–L4) and the sacral plexus (L4–S4). (The sacral plexus is discussed in Chapter 35.) The lumbar plexus consists of ventral rami from the L2 to L4 levels of the spinal cord, which exit the intervertebral foramina and course along the posterior abdominal wall, en route to the anterolateral abdominal wall and lower limb. The ventral rami are divided into anterior and posterior divisions, corresponding to the anterior (ventral) muscles (flexors) and the posterior (dorsal) muscles (extensors), similar to those in the brachial plexus (Figure 36-3B).
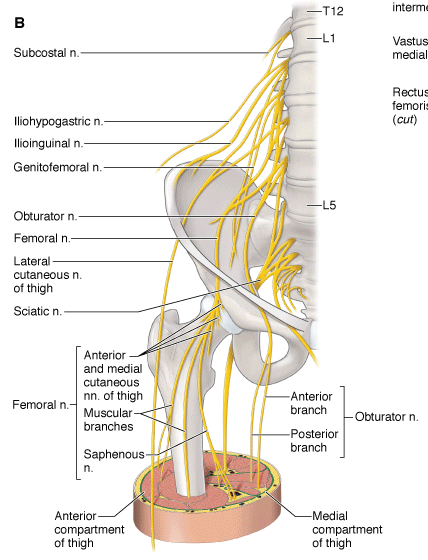
Branches from the lumbar plexus provide motor and sensory contributions not only to the anterior and medial compartments of the leg but also to the abdominal wall and pelvic areas. Branches are summarized as follows:
- Iliohypogastric and ilioinguinal nerves (L1). Emerge from the lateral border of the psoas major muscle and pierce the transverse abdominus muscle. The iliohypogastric and ilioinguinal nerves course anteriorly between the transverse abdominus and the internal oblique muscles, contributing to the motor innervation of the muscles of the abdominal wall (internal oblique and transversus abdominus muscles). In addition, the iliohypogastric nerve provides sensory innervation to the pubic region and the posterolateral gluteal skin. The ilioinguinal nerve (L1) provides sensory innervation to the superior medial thigh, root of the penis, anterior scrotum, mons pubis, and the labium majus.
- Genitofemoral nerve (L1–L2). Pierces the psoas major muscle and divides into two branches, the genital branch and the femoral branch. The genital branch enters the deep inguinal ring, providing motor innervation to the cremasteric muscle (male only) and sensory innervation to the skin of the anterior scrotum (or mons pubis) and the labium majus. The femoral branch passes behind the inguinal ligament to enter the femoral triangle, providing sensory innervation to the skin over the femoral triangle (superior and anterior region of the thigh).
The lumbar plexus is divided into posterior and anterior divisions, according to posterior and anterior muscle groups (Figure 36-3C).
- Posterior division
- Lateral cutaneous nerve of the thigh (L2–L3). Emerges from the lateral border of the psoas major muscle, crossing the iliacus muscle, and enters the thigh just medial to the anterior superior iliac spine, providing sensory innervation to the lateral thigh.
- Femoral nerve (L2–L4). Emerges as the largest branch of the lumbar plexus, deep to the lateral border of the psoas major muscle, and passes deep to the inguinal ligament. The femoral nerve then enters the anterior compartment of the thigh, where it provides motor innervation to the quadriceps femoris muscle group, the sartorius muscle, and part of the pectineus muscles. In addition, the femoral nerve provides sensory innervation via the following sensory branches:
- Anterior and medial cutaneous nerve of the thigh. Branches off the femoral nerve and supplies the skin of the anterior and medial thigh.
- Saphenous nerve. Branches off the femoral nerve and courses with the femoral artery and vein into the adductor canal. The femoral artery and femoral vein traverse the adductor hiatus and enter the popliteal fossa. In contrast, the saphenous nerve exits the adductor canal and supplies the skin on the medial region of the leg.
- Anterior division
- Obturator nerve (L2–L4). Emerges from the medial border of the psoas major muscle, passing posterior to the common iliac artery, and enters the medial compartment of the thigh through the obturator foramen. The obturator nerve provides motor innervation to the medial compartment of the thigh (excluding the pectineus and hamstring portion of the adductor magnus muscle). In addition, the obturator nerve provides sensory to the medial region of the thigh.
The blood supply to the lower extremity initiates from the descending aorta, which divides into the common iliac arteries. The common iliac arteries divide into the external and internal iliac arteries. The external iliac artery passes deep to the inguinal ligament to become the femoral artery, serving as the primary blood supply to the lower limb. The internal iliac artery gives rise to the obturator artery, which also contributes to blood supply of the lower limb.
Branches from the internal iliac artery exit the pelvis through the obturator foramen and bifurcate into anterior and posterior divisions. The two divisions circle the obturator foramen and supply blood, proximally, to the muscles inserting in the area. In addition, a branch enters the hip joint at the acetabular notch and travels through a conduit in the ligament of the head of the femur to supply blood to the femoral head.
Several arteries originate from the femoral artery, including the following (Figure 36-4A and B):
- Deep artery of the thigh (profunda femoris artery). The largest branch of the femoral artery. The deep artery of the thigh branches posteriorly in the femoral triangle and travels between the adductor longus and brevis muscles and the adductor longus and magnus muscles. Perforating branches of the deep artery of the thigh pierce through the adductor magnus muscle and are the major supplier of blood to the three compartments of the thigh. Distally, the deep artery of the thigh anastomoses with branches of the popliteal artery. Other branches that originate from the deep artery of the thigh include the following:
- Lateral circumflex femoral artery. Branches from the lateral side of the deep artery of the thigh (sometimes directly from the femoral artery) and travels laterally to branch into ascending, transverse, and descending branches.
- Ascending branch. Ascends deep to the tensor fasciae latae muscle and connects with the medial femoral circumflex artery.
- Transverse branch. Pierces the vastus lateralis muscle and wraps around the proximal shaft of the femur to anastomose with other vessels (i.e., medial femoral circumflex artery) to supply blood to the proximal femur and hip.
- Descending branch. Descends laterally and pierces the vastus lateralis muscle. The descending branch distally connects with the popliteal artery.
- Medial circumflex femoral artery. Branches medially from the deep artery of the thigh (may branch from femoral artery) and passes around the shaft of the femur. The medial circumflex femoral artery and branches of the lateral circumflex femoral artery supply the hip joint.
- Lateral circumflex femoral artery. Branches from the lateral side of the deep artery of the thigh (sometimes directly from the femoral artery) and travels laterally to branch into ascending, transverse, and descending branches.

A. Vasculature of the thigh. B. Femoral artery and its branches.
The main trunk of the femoral artery follows the adductor canal distally. It travels through an opening in the distal attachment of the adductor magnus (adductor hiatus) muscle and enters the popliteal fossa (posterior to the knee) to become the popliteal artery.
 Coronary angioplasty is a procedure that is frequently performed on patients who have obstructed blood flow to the heart musculature or who are experiencing a myocardial infarction. The femoral triangle allows easy access to a major blood vessel, the femoral artery. Because of the easy access, small balloons can be threaded through the femoral artery, at the femoral triangle, to coronary vessels in the heart. The balloon is then expanded to open the blood vessel.
Coronary angioplasty is a procedure that is frequently performed on patients who have obstructed blood flow to the heart musculature or who are experiencing a myocardial infarction. The femoral triangle allows easy access to a major blood vessel, the femoral artery. Because of the easy access, small balloons can be threaded through the femoral artery, at the femoral triangle, to coronary vessels in the heart. The balloon is then expanded to open the blood vessel.
The popliteal artery is the continuation of the femoral artery after it traverses the adductor hiatus (Figure 36-4A and B). The branches form an anastomotic vascular supply to the knee and are named according to their relationship to each other (superior lateral and medial genicular arteries and inferior lateral and medial genicular arteries).
The lymphatics of the thigh are organized into the following inguinal lymph nodes:
- Superficial inguinal nodes. Nine to eleven nodes that run parallel and distal to the inguinal ligament. The superficial inguinal nodes receive lymph from the external genitalia, anal canal, gluteal region, and the inferior abdominal wall; they receive most of the lymph from the superficial vessels of the lower limb. The superficial inguinal nodes drain to the external iliac nodes.
- Deep inguinal nodes. One to three nodes located medial to the femoral vein. The deep inguinal nodes receive lymph from deep vessels associated with the femoral vessels and glans penis or clitoris. Also, the deep inguinal nodes drain into the external iliac nodes.
- Popliteal nodes. Six small nodes located in the popliteal fat. The popliteal nodes receive lymph from the knee and the deep vessels associated with the tibial vessels of the leg. Vessels from the popliteal nodes ascend the thigh to drain into the deep inguinal nodes, eventually reaching the external iliac nodes.
The veins of the thigh consist of a superficial and a deep venous system. The superficial system consists of the great saphenous vein.
- Great saphenous vein. Originates from the dorsal venous arch in the foot on the medial side. The great saphenous vein ascends the leg and thigh on the medial side and pierces the fascia latae of the thigh, forming the saphenous opening to drain in the femoral vein.
- The deep venous system consists of as many as three veins that course with each artery. Most of the veins in the thigh drain into the femoral vein.
The knee complex consists of articulations between the femur and the tibia (tibiofemoral joint) and between the femur and the patella (patellofemoral joint). These articulations allow for static positions (standing) and dynamic movements (walking or running). The superior tibiofibular joint is not considered as part of the knee complex because it does not have the same capsule and is biomechanically linked with the ankle
The knee is composed of the following joints:
- Tibiofemoral joint. A synovial bicondylar joint with two degrees of motion. Articulations occur between the two condyles of the femur and the two tibial plateaus, producing flexion and extension. In addition, the tibiofemoral joint allows for minimal axial rotation with the pivot point, located medially on the medial tibial plateau.
- Patellofemoral joint. Articulation is between the intercondylar notch of the femur and the patella and shares the same joint capsule as the tibiofemoral joint. The patellofemoral joint directly serves the tibiofemoral joint; however, because of the vast differences in clinical problems and pathologies, the two joints will be discussed independently.
Patellofemoral disorder is one of the most common knee disorders seen in patients who visit orthopedic clinics. The disorder is usually caused by excessive pressure or malalignment between the patella and the femur, resulting in pain at the patellofemoral joint.
Ligamentous and Capsular Support of the Knee
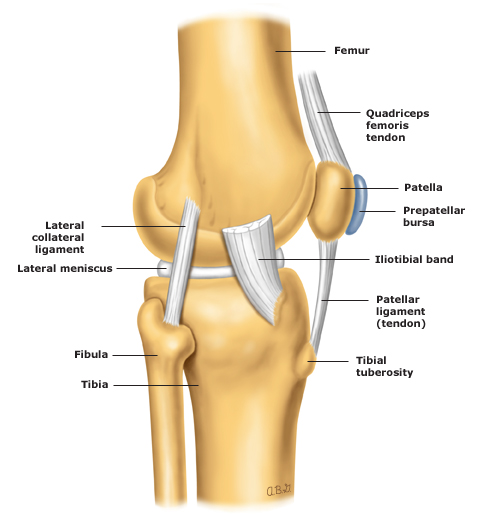
Ligament and capsule support of the knee are critical because of the incongruence of the joint, weight bearing of the joint, and the large range of motion with flexion and extension (Figure A–C). The ligaments and capsule provide support to the knee joint, as follows:
- Capsule. Surrounds the knee joint and includes the patellofemoral joint. The capsule extends from the distal femur to the proximal tibia and contains areas of laxity and recesses to allow for range of motion. The ligaments that support the capsule on all four sides of the joint are as follows:
- Oblique popliteal ligament. Supports the posterior capsule and attaches from the posteromedial tibial condyle to the center of the posterior capsule.
- Arcuate ligament. Supports the posterior capsule and attaches from the posterior fibular head to the intercondylar area of the tibia and the lateral epicondyle of the femur.
- Medial collateral ligament (tibial collateral ligament). Resists valgus forces on the knee (tibia abducting on femur). The medial collateral ligament attaches from the medial epicondyle of the femur to the tibial condyle and proximal shaft. In addition, it has an attachment to the medial meniscus.
- Lateral collateral ligament (fibular collateral ligament). Resists varus forces on the knee (tibia adducting on the femur). The lateral collateral ligament appears as a strong cord and attaches from the lateral femoral epicondyle to the fibular head.
- Patellar ligament. Attaches from the patella to the tibial tuberosity on the proximal anterior surface of the tibia. In addition, superficial fibers of the patellar ligament fan out, attaching to the sides of the tibial tuberosity. These structures are referred to as the medial and the lateral patella retinacula. The patellar ligament transmits forces produced by the quadriceps muscles to the tibia.

A. Anterior view of the right knee joint with the joint capsule open showing the patella reflected inferiorly. Posterior (B) and superior (C) views of the right knee joint.
In addition to the capsular ligaments, the knee complex also contains ligaments inside the capsule, called the cruciate ligaments. The cruciate ligaments are named by their location of attachment on the tibia.
- Anterior cruciate ligament. Attaches on the anterior intercondylar area of the tibia. The anterior cruciate ligament (known as the ACL) twists on itself as it ascends in a posterolateral direction to attach on the posteromedial side of the lateral femoral condyle. The ACL resists anterior translation of the tibia on the femur or posterior translation of the femur on the tibia.
- Posterior cruciate ligament. Stronger than the ACL and attaches to the posterior intercondylar area of the tibia. The posterior cruciate ligament ascends in an anteromedial direction to attach on the lateral surface of the medial femoral condyle. The posterior cruciate ligament resists posterior translation of the tibia on the femur or anterior translation of the femur on the tibia.
Menisci of the Knee Joint
The knee contains two fibrocartilaginous structures, one over the medial tibial plateau, the medial meniscus, and one over the lateral tibial plateau, the lateral meniscus (Figure A–C). Both are crescent shaped and do not complete a full circle. The menisci are also wedge shaped and, medially, are thin. However, laterally, the menisci are thicker, which increases the concavity of the articulating surface of the tibia.
- Medial meniscus. The anterior portion of the medial meniscus attaches to the anterior intercondylar area of the tibia and the posterior portion to the posterior intercondylar area. Its peripheral border is attached to the capsule, and a portion is attached to the medial collateral ligament.
- Lateral meniscus. Forms four-fifths of a complete circle. The anterior portion of the lateral meniscus attaches to the anterior intercondylar area of the tibia, and the posterior portion attaches to the posterior intercondylar area.
A tear of the ACL is usually seen in patients who participate in sports that require cutting movements with deceleration (e.g., soccer, football). The mechanism of injury is usually deceleration of the body on an outstretched leg with lateral rotation of the femur on a fixed tibia. Treatment is often surgery using an autograft (i.e., tissue is taken from the patient to replace the patient's ligament). Frequently, a midpatellar ligament graft is used.
Bursae Associated with the Knee Joint Complex
The knee joint has many bursae (sacs of synovial fluid) to decrease frictional forces. The most important bursae are as follows:
- Suprapatellar bursa. Located between the quadriceps tendon and the anterior femur.
- Subpopliteal bursa. Located between the popliteus muscle and the lateral femoral condyle.
- Gastrocnemius bursa. Located between the medial head of the gastrocnemius muscle and the medial femoral condyle.
- Prepatellar bursa. Located between the skin and the anterior patella.
- Subcutaneous infrapatellar bursa. Located between the patellar ligament and the tibial tubercle.
Prepatellar bursitis (commonly known as “housemaid's knee”) is caused by inflammation or bursitis of the superficial infrapatellar bursa between the skin and the patellar ligament. The mechanism of injury can be from direct impact or from an irritation to the knee that occurs over time. The condition is often seen in individuals whose occupations require them to place pressure on the knees, such as carpet layers or people who wash the floor on their hands and knees (thus the term housemaid's knee), resulting in pain over the patellar ligament.
While operating on the posterior compartment of the thigh, an orthopedic surgeon takes care to preserve the arterial blood supply to the muscles in that region. These are branches of which of the following arteries?
The correct answer is A.
The blood supply to the posterior compartment of the thigh originates from perforating branches of the deep femoral artery.